classic Hodgkin lymphoma
   Expand All
Expand All | Collapse All
Clinical- 95% of all Hodgkins
- bimodal age peaks 15-35, then elderly
- associations: mono
- site: cervical nodes (75%), other nodes, mediastinal involvement (60%), splenic involvement (20%)
- stains and molecular same across all subtypes
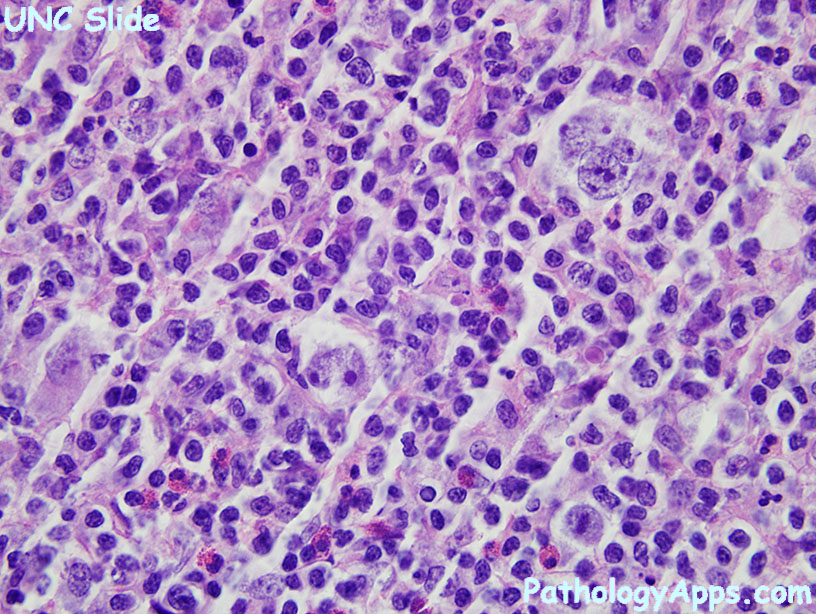
Histology- Mononuclear Hodgkin cells
- Reed Sternberg cells
- large, resembles CMV
- at least 2 nuclei or lobes
- prominent nucleoli
- pale chromatin
- Mummified cells
- pyknotic reddish nuclei
- condensed cytoplasm
- Background mixed inflammatory cells
Subtypes- nodular sclerosing
- 70% of classical Hodgkins
- nodules surrounded by thick collagen
- lacunar cells (artifact causing clearing around Hodgkin cells)
- background eosinophils and histiocytes
- lymphocyte rich
- 5% of classical Hodgkins
- nodular with germinal centers (CD21), rarely diffuse
- no fibrosis, PMNs or eosinophils
- RS cells are rarer, NLP-like, and found in mantle zones
- mixed cellularity
- 20% of classical Hodgkins
- diffuse, background eosinophils
- most association with EBV
- doesn't fit other types
- lymphocyte depleted
- <1% of classical Hodgkins
- HIV association, prefers retroperitoneal nodes
- diffuse +/- fibroblasts
- predominance of Reed Sternberg cells
- paucity of lymphocytes, lack eosinophils
Stains- Stain Reed Sternbergs
- positive: CD30, CD15, weak PAX5
- negative: CD20 (or weak), CD45, J chain, CD75, macrophage markers, CD138
- EBV variable, high in 3rd world
- CD30 normally stains grans, plasma cells, activated lymphs, NKs, monos
- CD15 normally stains myeloid cells, eos, activated lymphs
Molecular- same across subtypes
- clonal IG rearrangement
- NFkB activation -> JAK/STAT
- cytokine causes inflammatory cells
|